
This year's ASCO conference in Chicago, which drew more than 40,000 participants, made headlines around the world after showcasing a series of groundbreaking studies. One presentation — a revolutionary treatment for pancreatic cancer that doubled the survival time of people with the disease — even received a spontaneous standing ovation from the audience. The achievement was made possible thanks to several innovative advances in cancer treatment, including targeted therapies aimed at specific genes or proteins, personalized cancer vaccines, and treatments using patients' own immune cells. Artificial intelligence is playing a major role in this progress, dramatically reducing the time needed to discover new drugs.
ASCO sensation: breakthroughs in stomach and lung cancer treatment
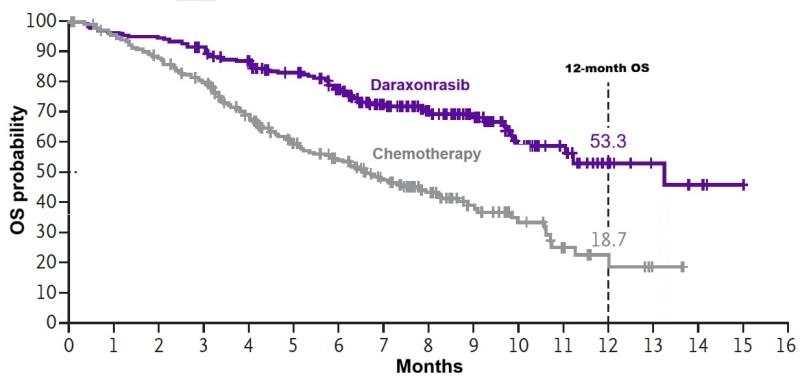
Pancreatic cancer is among the most difficult types to treat. According to the American Cancer Society, the overall five-year relative survival rate across all subtypes is about 13%. But around 90% of pancreatic tumors harbor a mutated KRAS gene, a biomarker that can be targeted with precision medicine. At the 2026 ASCO conference, researchers presented a study showing that overall survival in patients with pancreatic cancer doubled with daraxonrasib therapy. The drug also halted or reversed tumor growth significantly more often than standard treatment, benefiting 33% of patients with cases featuring this mutation, compared with 11% receiving conventional therapy.
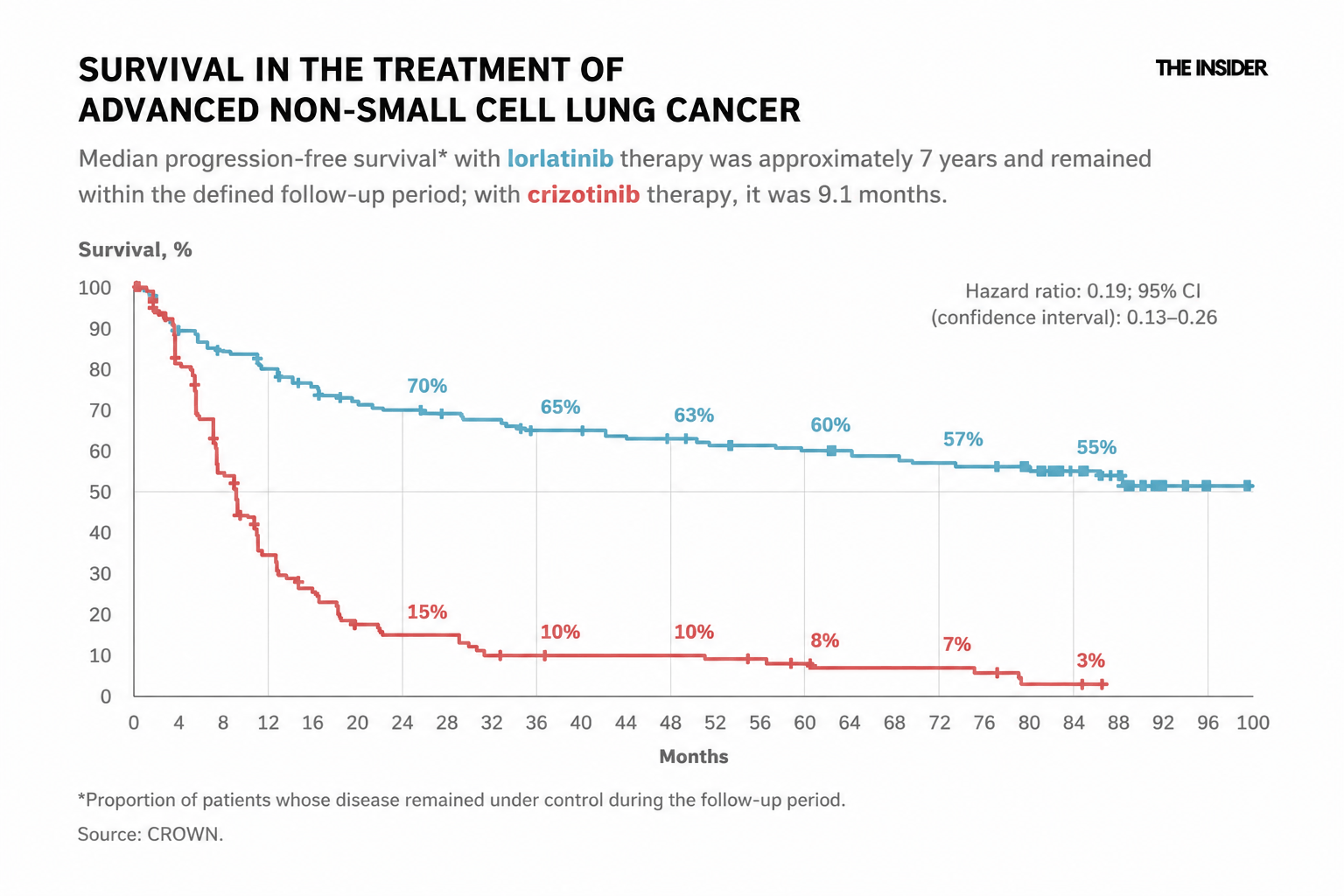
At the same conference, researchers presented other striking results for targeted therapy, this time involving lorlatinib for patients with ALK-positive non-small cell lung cancer (NSCLC). NSCLC accounts for approximately 80–85% of all lung cancer cases, according to the American Cancer Society. However, the ALK-positive subtype is relatively rare, occurring in only about 3–5% of patients, according to a review published in Cancers. Lorlatinib achieved a seven-year overall survival rate exceeding 50%, compared with just 3% for patients receiving the previous-generation drug.
Both studies achieved these results thanks to advances in targeted therapy, one of the most successful developments in oncology in recent years.
How targeted therapy works
Cancer is often classified by the tissue in which it originates, such as the lung or breast. However, it has long been known that cancers arising in the same tissue may be driven by tumors with entirely different genetic mutations, protein profiles, cellular programs, tumor microenvironments, and clinical behavior. Moreover, tumors can differ not only between patients but also between different regions of the same tumor and between the primary tumor and its metastases. A review published in Nature Reviews Clinical Oncology describes this remarkable molecular diversity.
Conventional chemotherapy works indiscriminately, attacking cells that divide more rapidly than others. But several healthy tissues in the body also renew themselves quickly, including the lining of the mouth and intestines, hair follicles, and bone marrow. As a result, these tissues are damaged alongside the tumor, causing familiar side effects such as nausea, mouth ulcers, hair loss, and impaired blood cell production. Targeted drugs take a more precise approach by attacking specific molecular targets, known as biomarkers. Increasingly, oncologists begin by asking what is happening inside the tumor itself. This assessment, known as biomarker testing, looks for genes, proteins, and other characteristics in a tumor sample that can help determine which treatment is most likely to benefit a particular patient. The role of these biomarkers is explained by the U.S. National Cancer Institute in its overview of tumor markers. Two people with the same type of cancer may therefore require different treatments due to the fact that their tumors differ at the molecular level.
Even a single tumor can resemble a mosaic. Cells in different regions may have distinct appearances, rely on different molecular pathways for growth, and respond differently to treatment. A striking example is lung adenocarcinoma, in which different areas within the same tumor sample can exhibit different tissue structures, molecular characteristics, and patterns of gene activity. This diversity arises due to the fact that tumors are constantly evolving. As cancer cells divide, they accumulate new genetic mutations, while the DNA repair systems in many tumors function less effectively than in normal cells. Additional differences emerge through changes in gene and protein activity, meaning that cells with nearly identical DNA can activate different programs that regulate growth, survival, and migration.
The tissue surrounding a tumor also influences its behavior. Fibroblasts, immune cells, and blood vessel cells in the tumor's immediate environment release signaling molecules that can accelerate cancer growth, help tumor cells invade neighboring tissues, or enable them to survive treatment. As a result, the tumor gradually develops into a complex ecosystem of cells with different characteristics and varying sensitivity to therapy, as described in this review.
The first targeted therapies emerged around the turn of the century. One of the earliest was imatinib, a drug developed to treat chronic myeloid leukemia (CML), a disease in which blood cells receive a continuous growth signal from an abnormal BCR-ABL protein — imatinib was specifically designed to block that signal. In 2001, the U.S. Food and Drug Administration (FDA) approved imatinib for patients with Philadelphia chromosome-positive chronic myeloid leukemia. Years later, it became clear just how dramatically the drug had changed the disease's prognosis. According to a long-term study cited by the U.S. National Cancer Institute, patients who remain in remission after two years of imatinib therapy have a life expectancy comparable to that of people of the same age in the general population.
A similar transformation occurred in the treatment of breast cancer. In some patients, tumors produce excessive amounts of the HER2 protein, which promotes cell growth and division. In 1998, the FDA approved trastuzumab (an antibody that targets HER2) for the treatment of HER2-positive metastatic breast cancer. It was one of the earliest examples of a therapy selected not simply according to the organ affected, but according to the tumor's molecular characteristics.
Not just targeted therapy: what else ASCO 2026 revealed
Targeted therapy is no longer the only path toward precision cancer treatment. At the ASCO 2026 annual meeting in Chicago, researchers presented a wide range of promising advances in oncology. Although these approaches differ in how they work, they all share the same underlying principle: first identify a tumor's unique vulnerability, then design a treatment specifically to exploit it.
Personalized mRNA cancer vaccines
The word “vaccine” is usually associated with disease prevention, but in oncology it refers to a therapeutic treatment given to people who already have cancer. This approach is individualized and highly specific. Doctors first obtain a sample of the patient's tumor, analyze its mutations, and create a vaccine targeting molecular features that are unique to the cancer and absent from healthy cells. The vaccine then trains the immune system to recognize and attack the tumor.
One of the biggest announcements at ASCO 2026 was the five-year follow-up of the personalized mRNA vaccine Intismeran Autogene (mRNA-4157), developed by Moderna and Merck. In patients with high-risk melanoma, the vaccine can be combined with the immunotherapy pembrolizumab to reduce the risk of recurrence or death by 49%, and maintain the benefit over five years of follow-up. The vaccine is now being evaluated in large Phase III clinical trials for melanoma, lung cancer, and kidney cancer.
CAR-T therapy reaches solid tumors
CAR-T therapy uses a patient's own immune cells as treatment. Doctors collect immune cells from the patient, genetically engineer them in the laboratory so they can recognize cancer cells, and then infuse them back into the body. In effect, the treatment itself is a living drug. For many years, this approach proved highly effective against blood cancers but was largely unsuccessful against solid tumors.
On June 24, 2026, China's National Medical Products Administration approved Satricel, developed by CARsgen, for the treatment of gastric cancer, making it the world's first CAR-T therapy approved for a solid tumor. In clinical trials, the treatment roughly doubled the length of time before the disease began progressing again. The approval demonstrated for the first time that engineered immune cells can be successfully adapted to target solid tumors that had previously resisted this form of therapy.
An antibody that delivers medicine directly to the tumor
This approach has a long technical name — an antibody-drug conjugate (ADC) — but the concept is straightforward. The antibody acts as a navigator, locating the cancer cell on its own. Attached to it is a drug payload that is released only after the antibody enters the cell, allowing the treatment to attack the tumor while largely sparing healthy tissues.
At ASCO 2026, researchers presented results for sacituzumabgovitecan. In patients with triple-negative breast cancer, a disease that is notoriously difficult to treat, the drug kept the cancer under control for significantly longer than standard chemotherapy: about 11 months versus 8 months when used in combination with immunotherapy. Another experimental drug, Izabren, the world's first dual-target “navigator” directed at both EGFR and HER3, produced responses in nearly half of patients with lung cancer.
Striking the RAS target once considered “undruggable”
Mutations in the RAS gene are found in many types of cancer, yet for decades researchers were unable to develop drugs capable of targeting them. The protein was widely regarded as “undruggable.” Daraxonrasib, discussed above in the section on pancreatic cancer, is among the first drugs to overcome this obstacle. According to the study presented at ASCO 2026 and published in the New England Journal of Medicine, it marks the beginning of a new generation of pan-RAS inhibitors that can finally attack this long-elusive target. If these findings are confirmed in larger clinical trials, they could offer an effective treatment option to patients who previously had few, if any, therapeutic alternatives.
Detecting tumors through a blood test
To strike a tumor's weak point with precision, doctors first have to find it. That is why diagnosis has become just as important as selecting the right therapy. One of the fastest-growing advances in oncology is the liquid biopsy — a blood test that detects fragments of tumor DNA circulating in the bloodstream. These fragments can help doctors choose an appropriate targeted therapy and, in the future, may allow cancers to be detected before they become visible on medical imaging. At ASCO 2026, liquid biopsy emerged as one of the conference's central themes. Dozens of presentations explored evidence that the test can not only predict patient outcomes but also guide treatment decisions, helping physicians determine when therapy should be intensified — or, conversely, de-escalated. In one study, for example, measuring circulating tumor DNA at the end of lymphoma treatment predicted relapse more accurately than conventional PET/CT imaging.
Vaccines, engineered immune cells, antibody “navigators,” and molecules designed with the help of artificial intelligence may seem like a diverse collection of technologies. Yet they all follow the same principle as lorlatinib and daraxonrasib: identify the tumor's specific vulnerability and attack it with precision. Only the method of attack differs.
The 2026 ASCO meeting revealed a wealth of new ways to do exactly that. Participants noted that the conference was among the most practice-changing in recent years, with an unusually large number of presentations reporting results that have the potential to reshape the standards of cancer care.
Artificial intelligence in the fight against cancer
Artificial intelligence is increasingly doing more than simply screening existing molecules — it is designing entirely new ones and identifying the biological targets they should attack. The first major proof that this approach works was published in Nature Medicine in 2025. Rentosertib, developed by Insilico Medicine, was designed by AI to attack a molecular target that the AI itself had previously identified. The drug successfully completed an early-stage clinical trial. Although rentosertib was developed to treat pulmonary fibrosis rather than cancer, the study demonstrated that the AI-driven drug discovery approach is viable. Another company attracting close attention is Isomorphic Labs, a Google DeepMind spinout created by the team behind AlphaFold, the AI system that revolutionized protein structure prediction. The company expects to begin the first clinical trials of its AI-designed cancer drugs by the end of 2026.
Artificial intelligence is increasing the speed of evolution in target therapy. Precision oncology depends on integrating data from genomics, transcriptomics, proteomics, and clinical practice — AI can rapidly identify hidden patterns across these datasets and match a tumor's molecular profile with the most appropriate treatment strategy. Platforms such as Watson for Genomics and similar systems analyze genomic alterations together with the latest medical research to recommend targeted drugs and drug combinations tailored to specific mutations.
Today, AI has become one of the central tools not only in targeted therapy but in oncology as a whole. It helps detect cancer earlier, select more effective treatments, and support patients throughout the course of therapy. AI algorithms can analyze CT scans, MRI images, mammograms, and other medical images, identifying tiny tumors and precancerous changes that may escape the human eye. This improves the sensitivity of cancer screening for lung, breast, prostate, and several other cancers. Machine learning systems also compare a patient's medical history, imaging results, biopsy findings, and biomarkers with vast databases of clinical cases and treatment guidelines, producing therapeutic recommendations that have been shown to approach expert-level decision-making.
Given the rapid pace of AI development, next year's ASCO meeting is likely to showcase even more groundbreaking research.
