
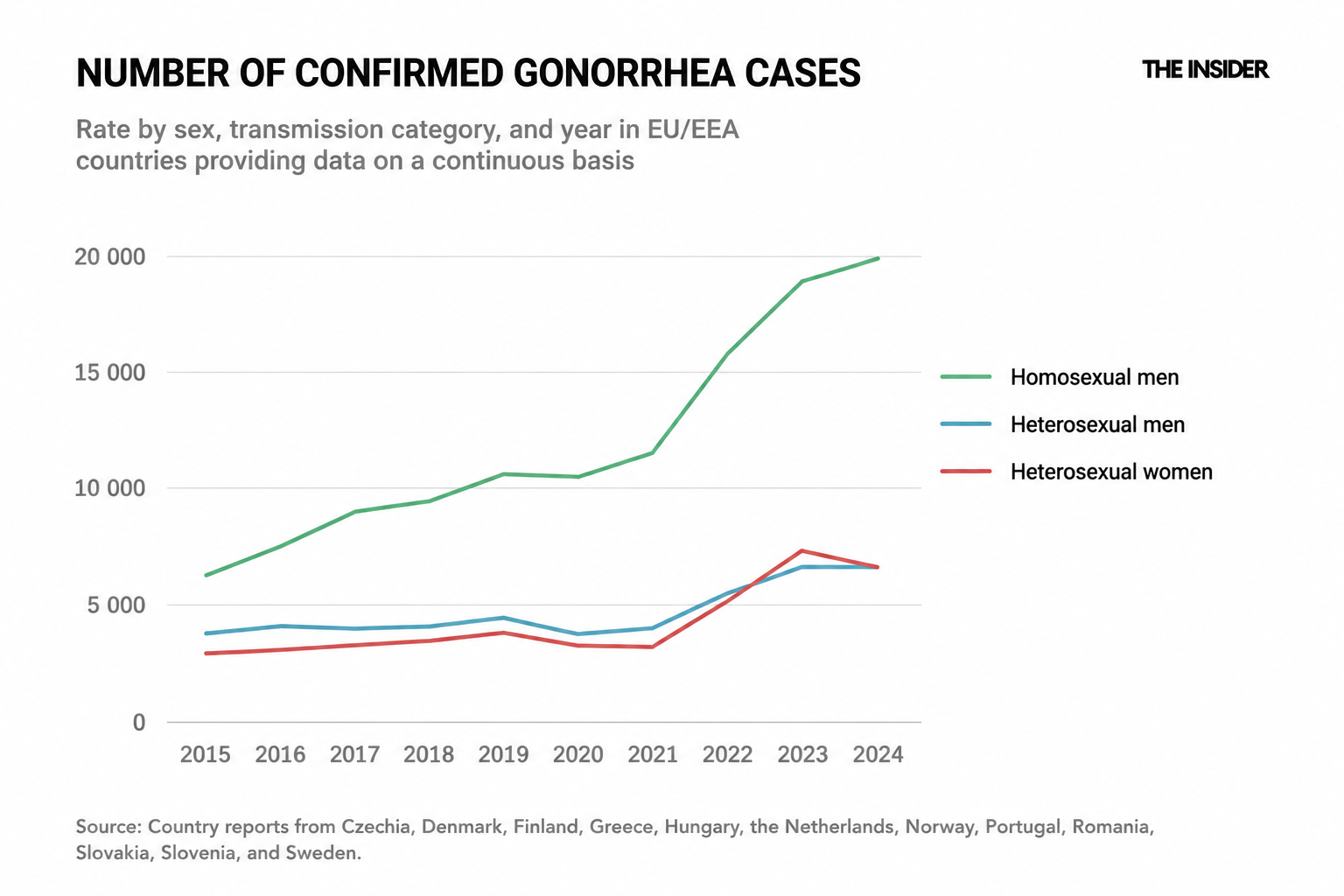
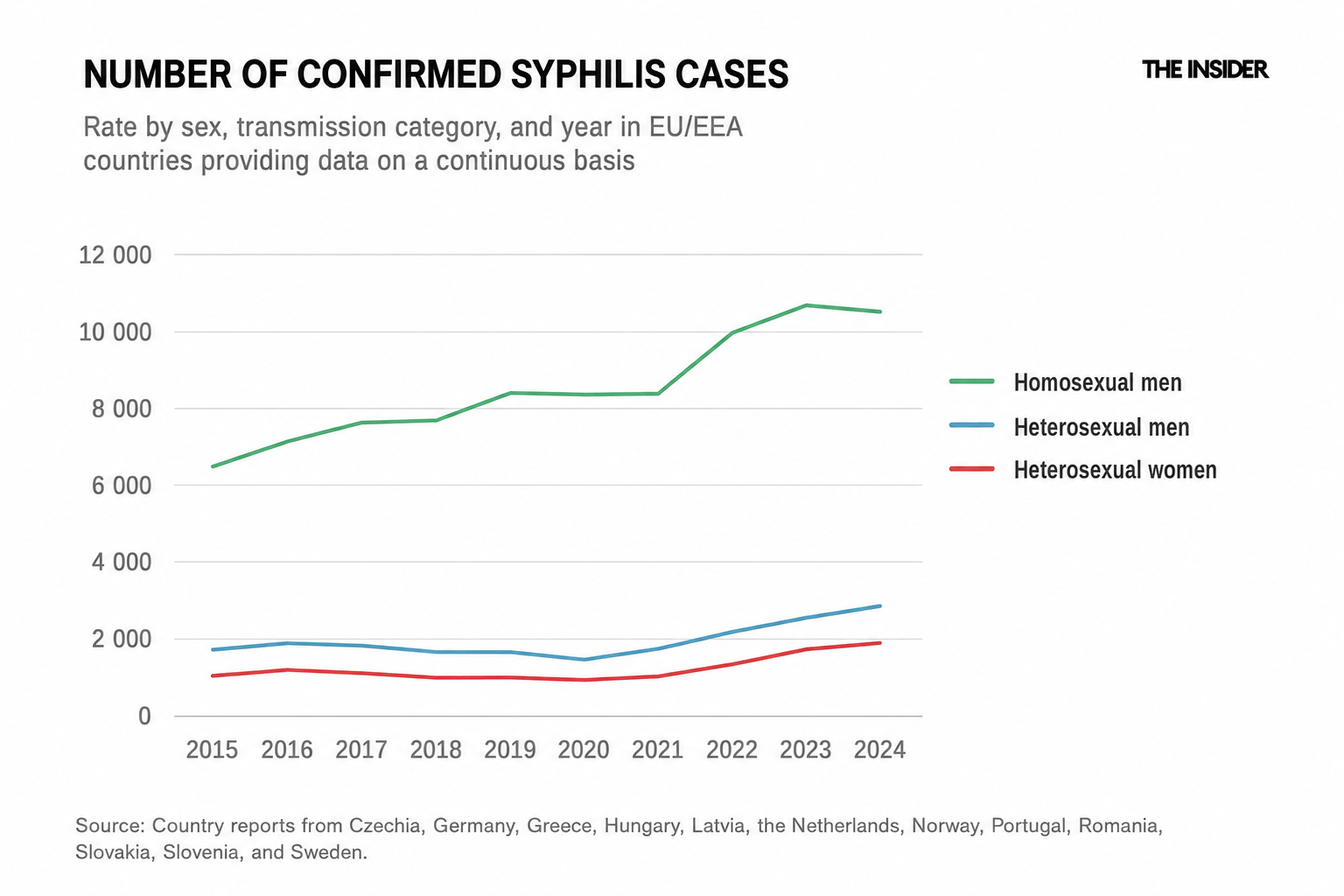
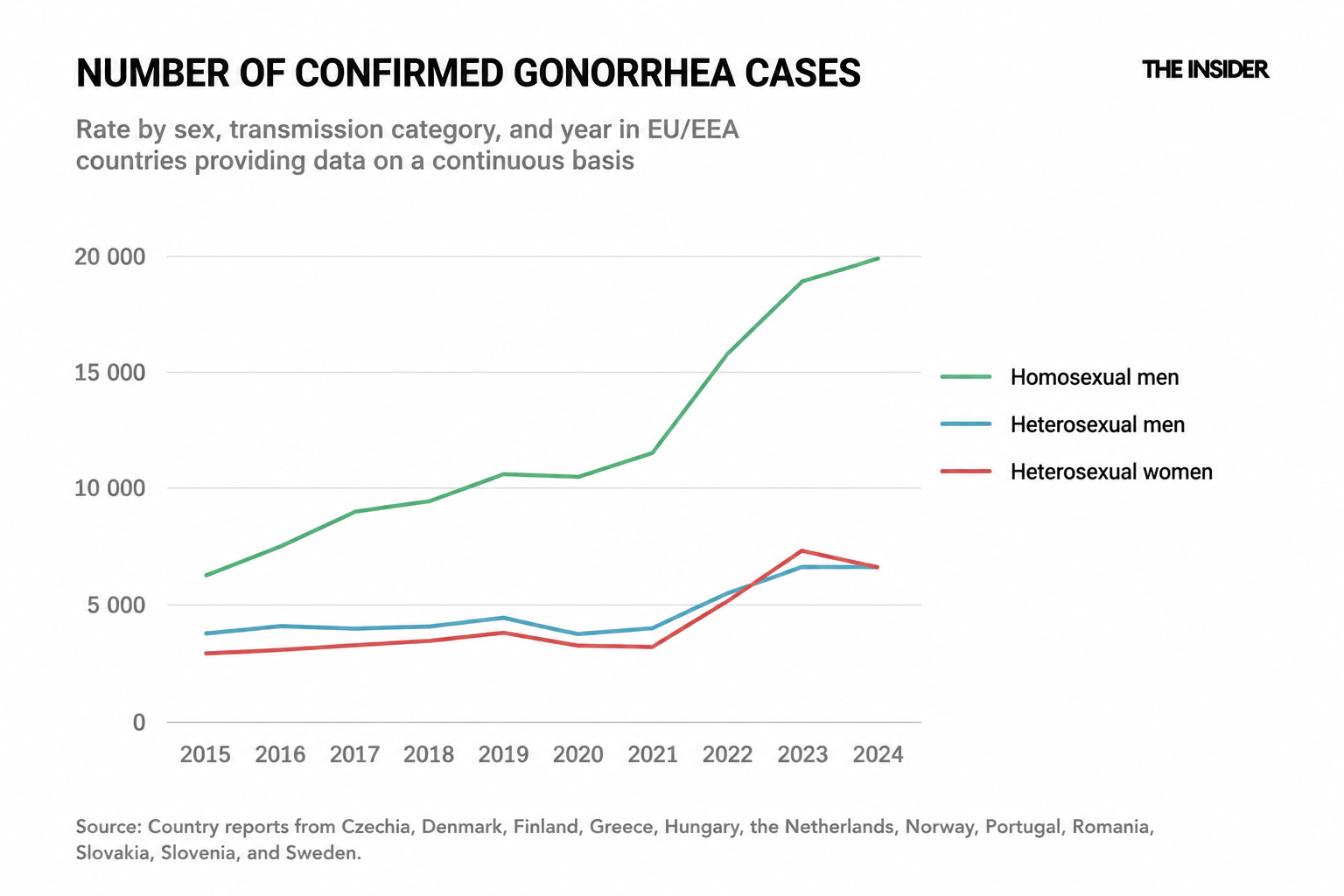
The European Centre for Disease Prevention and Control (ECDC) has reported a sharp increase in the spread of bacterial sexually transmitted infections (STIs). In 2024, the number of gonorrhea, syphilis, and congenital syphilis cases reached their highest levels since records began. Infections that until recently were considered virtually defeated are once again spreading rapidly across Europe. Several factors are driving the trend: the scaling back of prevention programs in some countries, changes in sexual behavior as fear of HIV has diminished, the growing popularity of psychoactive substances, reduced access to medications, and unequal access to healthcare in general.
Socioeconomic roots of STI epidemics
Historically, every major outbreak of syphilis and gonorrhea has coincided with war, mass migration, poverty, and other socioeconomic disruptions. One of the first large-scale syphilis epidemics swept across Europe at the end of the 15th century, coinciding with the Italian campaign of King Charles VIII of France in 1494–1495. Vast armies accompanied by mercenaries, merchants, and prostitutes created ideal conditions for the spread of infection.
During the Industrial Revolution of the 19th century, urban growth, population migration, and changing lifestyles were accompanied by a new wave of STIs. In major European cities, syphilis and gonorrhea affected between 5% and 20% of the population.
STIs were a particular concern for governments during wartime. During World War I, for example, venereal diseases sidelined 18,000 soldiers per day in the U.S. Army.
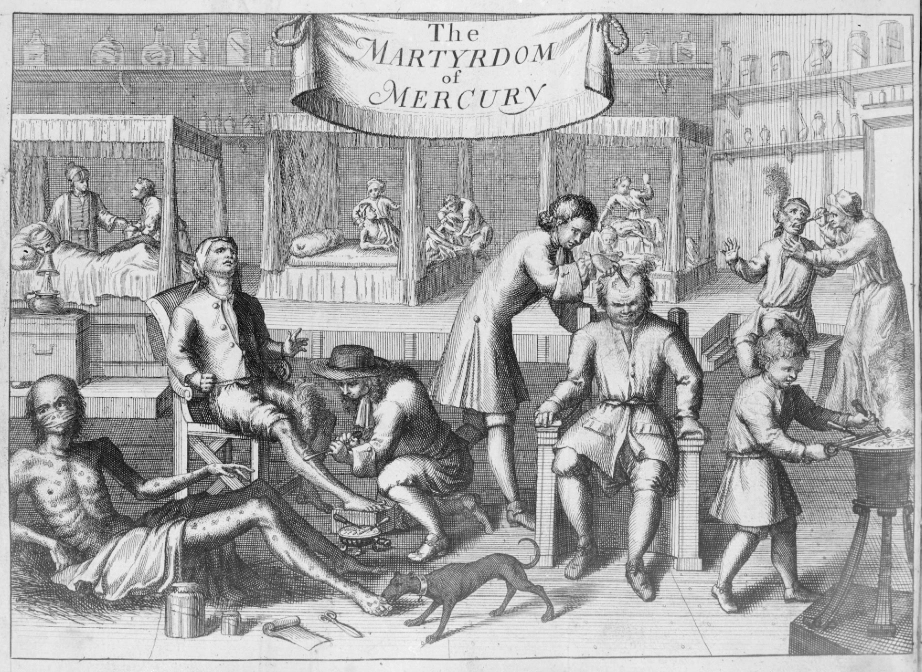
European states have long attempted to address the problem by restricting prostitution. Special registries were established, mandatory medical examinations were carried out, and infected people were isolated. Control and surveillance measures were directed primarily at women, who at the time were regarded as the main source of the problem. Men, despite playing a key role in spreading infection, were largely outside the reach of both public health surveillance and religious control. Because of the social and religious stigma attached to STIs, many affected people were reluctant to seek help, thereby contributing to the continued spread of disease.
In 1928, Alexander Fleming isolated penicillin, and in the 1940s, Oxford University scientists Howard Florey and Ernst Chain developed effective methods for its purification, paving the way for the drug's widespread medical use.
The advent of antibiotics proved decisive in the fight against bacterial infections, including STIs. As late as 1943, treatment for gonorrhea required a 30-day stay in a hospital, but by 1944 the course of treatment had been reduced to five days and could be administered without hospitalization.
As late as 1943, treatment for gonorrhea required a 30-day stay in a hospital, but by 1944 the course of treatment had been reduced to just five days
In the postwar decades, syphilis rates in Europe declined sharply, driven not only by the spread of antibiotics but also by the widespread adoption of contraception (particularly latex condoms), as well as the expansion of public healthcare systems. Large-scale testing and treatment programs were introduced, and the cost of medical care fell. Some countries also imposed criminal penalties for knowingly transmitting STIs. In the Soviet Union, and later in Russia, criminal liability exists for the intentional transmission of sexually transmitted infections.
Following the introduction of penicillin and the dramatic decline in infection rates after World War II, many came to believe that the problem of STIs was becoming a thing of the past. However, during the 1960s and 1970s, researchers began to document a renewed rise in STI incidence. Some scholars have linked this trend to sweeping changes in social norms, including a lower starting age for sexual activity and increased urban mobility.
The decline in STI rates during that period was also influenced by the HIV epidemic that swept across the world in the 1980s. The emergence of the deadly new infection dramatically increased public awareness of the risks of transmission. Many countries launched large-scale campaigns promoting safer sex, and condom use became significantly more widespread. As a result, the prevalence of certain STIs temporarily declined in some countries.
The situation in the Soviet Union was more tightly controlled. By the 1960s and 1970s, the country had developed an extensive network of dermatovenerology clinics and a system of mandatory epidemiological surveillance. The state actively traced the contacts of infected people, introduced long-term medical monitoring, and carried out mass preventive screenings. This model was rigid and largely incompatible with modern notions of medical confidentiality, but when it came to controlling infection rates it remained effective for many years.
The Soviet model was rigid and largely incompatible with modern notions of medical confidentiality, but it was effective
During the 1990s, Europe experienced an uneven epidemiological landscape with regard to STIs. Following the collapse of the socialist bloc and sweeping socioeconomic changes, countries across the region began to develop along different trajectories. The sharpest increase in syphilis rates was recorded in the former Soviet republics, particularly Russia, Ukraine, and Belarus.
Epidemiologists attributed this surge to several concurrent processes: rising poverty, mass migration, the breakdown of established healthcare systems, the reduction of prevention programs, and broader changes in social and living conditions.
In Western Europe, the situation was more favorable. During the first half of the 1990s, the Scandinavian countries — Sweden, Norway, Finland, and Denmark — experienced declining gonorrhea rates. By the end of the decade, however, researchers began to identify new pockets of growth in the United Kingdom as well as in the Netherlands.
Experts linked these developments not only to patterns of sexual behavior but also to differences in access to diagnostic services, the effectiveness of healthcare systems, and the quality of epidemiological surveillance. Some countries maintained robust systems of prevention and early detection, while others were undergoing profound social and economic transformations that were directly reflected in disease trends.
The end of fear of HIV
The current STI surge is the result of several independent processes overlapping with one another, each of which either altered people's behavior or weakened healthcare systems. Together, they have created the conditions for a sustained increase in infection rates that has now lasted for more than a decade.
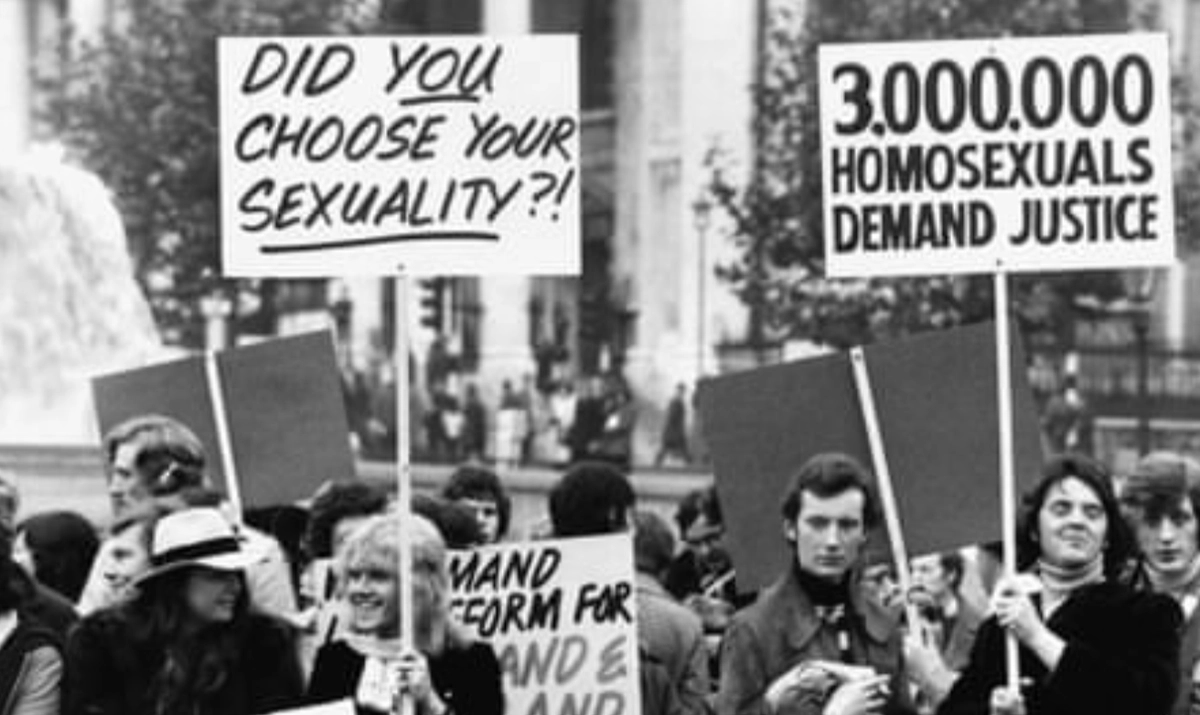
On June 5, 1981, the U.S. Centers for Disease Control and Prevention (CDC) published a brief report that changed the course of medical history. It told the story of five young, previously healthy gay men in Los Angeles who had developed a rare form of pneumonia, Pneumocystis carinii, which was virtually unseen in people with normal immune systems. Two of them had already died, and doctors did not understand what was happening. Reports of similar cases soon emerged from New York and San Francisco, and a year later the new disease was finally given a name: AIDS.
Emerging at the height of the sexual revolution, which had already transformed the intimate behavior of an entire generation, the mysterious virus triggered a wave of fear. The disease was killing young, healthy people, and there was no treatment. Governments launched large-scale campaigns promoting safer sex.
In 1986, U.S. Surgeon General Vice Admiral C. Everett Koop published a brochure explaining the very real risks of unprotected sex. In 1987 the United Kingdom released a special brochure targeting heterosexual teenagers — Love Carefully: Use a Condom — openly promoting condoms as a tool for protection against a disease.
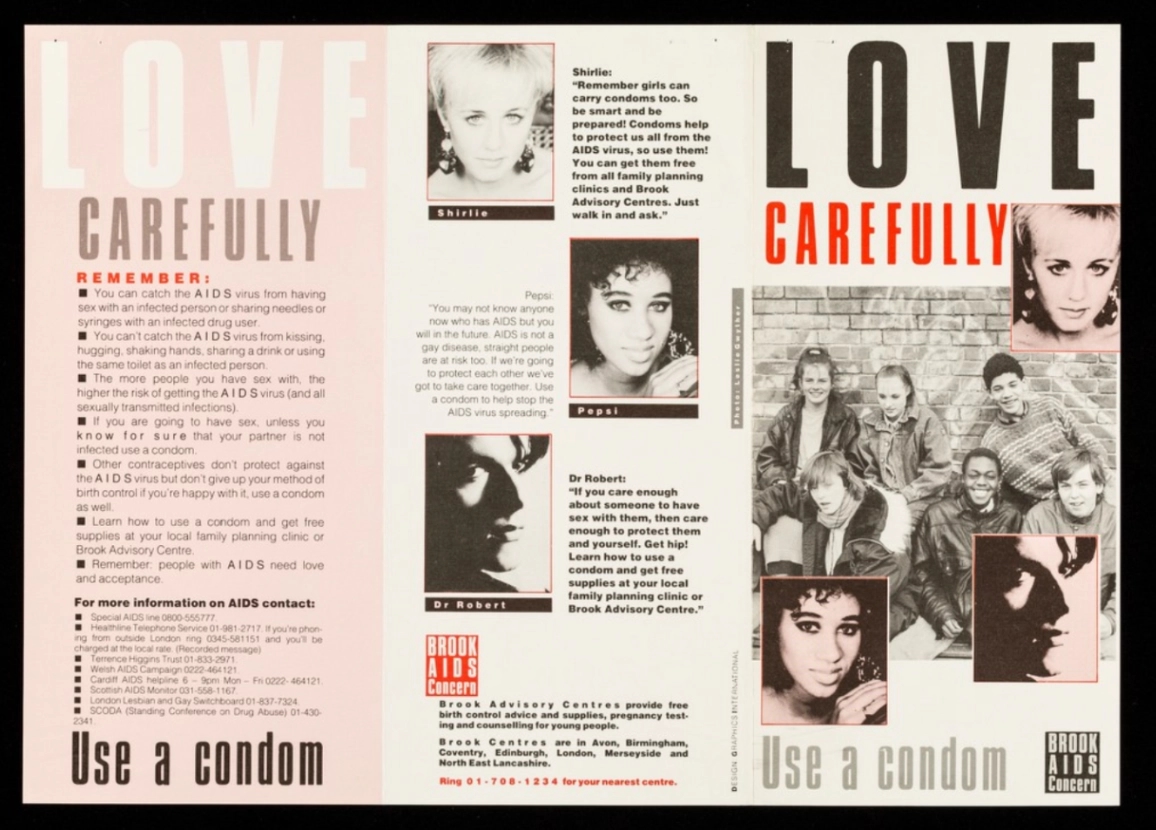
The impact of these campaigns was twofold. Their primary goal was to curb the spread of HIV, but they also helped reduce the incidence of other STIs. Prevention programs in the 1980s increased overall condom use by roughly 25%, as the fear of death proved to be a more powerful regulator of sexual behavior than any previous campaign against gonorrhea or syphilis.
Then, in 1996, everything changed with the advent of highly active antiretroviral therapy (HAART, or ART) for the treatment of HIV infection. Typically, the process combines three or four drugs that suppress viral replication, restore immune function, and transform HIV into a manageable chronic condition.
The arrival of ART was a medical triumph, but it simultaneously removed the principal behavioral deterrent: fear. This, in all likelihood, contributed to a renewed increase in the incidence of other sexually transmitted infections.
The advent of ART was a medical triumph that reduced fear of HIV and, in all likelihood, contributed to rising STI rates
As early as 2004, a group of Brazilian researchers led by Benoît Mâsse confirmed this mechanism through mathematical modeling. Between 0% and 55% of new bacterial STI cases could be attributed to the widespread adoption of ART within the population, driven by a relatively modest increase in risky behavior at the population level. In other words, even a small collective shift in behavior, multiplied across an entire population, can produce a substantial epidemiological effect.
"When was the last time you saw a large-scale government campaign promoting condoms as a means of protection against HIV and other STIs among men who have sex with men (MSM)?" researchers ask rhetorically. In their view, such campaigns have largely disappeared from public health agendas, meaning a new generation is growing up without fully appreciating the importance of safer sex.
HIV pre-exposure prophylaxis and “risk compensation”
The next turning point came with the advent of HIV pre-exposure prophylaxis (PrEP) — the preventive use of antiretroviral drugs by HIV-negative people to reduce the risk of acquiring the infection.
PrEP is widely used among men who have sex with men (MSM), sex workers, and HIV-negative partners of HIV-positive people. Researchers at the University of Melbourne documented a phenomenon known as “risk compensation” among PrEP users: reliable protection against HIV was accompanied by reduced condom use and rising STI rates.
Additionally, a Madrid study conducted between 2017 and 2019 among MSM found that risk compensation manifested primarily through less frequent condom use during anal sex, while the number of sexual partners and the use of psychoactive substances remained stable. At the same time, STI incidence within the group was very high, particularly for rectal gonorrhea and chlamydia.
However, the relationship cannot be reduced to a simple cause-and-effect link. Danish researchers led by Frederik Engsig conducted a cohort study between 2019 and 2022 and found that a 35% increase in STI incidence was associated with PrEP use, but the rise in cases began 10–20 weeks before participants started taking the medication. This suggests that people often seek PrEP not before, but during periods of increased sexual activity. In addition, PrEP tends to attract groups that already face a higher baseline risk of infection.
Chemsex
A closely related factor is the rise of chemsex — the deliberate use of psychoactive substances to enhance sexual experiences. Chemsex, as well as slamsex (the injection of psychoactive substances before sex), also increases the risk of STI transmission.
The trend is particularly evident in Spain. Researchers from Hospital Clínic de Barcelona estimated that 89% of PrEPusers reported using psychoactive substances, substantially higher than the figures from England (38.5%) and the Netherlands (41%). Austrian researchers found that, when compared with people who did not use psychoactive substances during sex, those who engaged in chemsex experienced higher rates of gonorrhea (38% versus 21%) and syphilis (17% versus 5%).
Funding cuts after the 2008 financial crisis
Alongside changes in behavior, public health response systems were also weakening. The 2008 financial crisis triggered a wave of cuts to public healthcare spending across Europe and North America just as the epidemiological burden was beginning to increase.
In the United Kingdom, reductions in funding for sexual health services resulted in the reduction in services from specialized clinics. Budget cuts also eliminated positions for contact tracers — specialists trained to notify and encourage the sexual partners of infected patients to undergo testing. Outreach services for high-risk groups — including sex workers and MSM — were likewise scaled back.
The post-COVID rebound
The COVID-19 pandemic created a brief illusion of improvement. In 2020, STI incidence fell sharply across Europe, primarily because of restrictions on movement and reduced access to diagnostic services. In reality, however, transmission appears not to have stopped during this period, but instead continued largely undetected. Once the restrictions were lifted, reported case numbers began to climb rapidly.
Actual transmission of infection during the COVID-19 pandemic appears not to have stopped but simply went undetected
In 2021, for example, Spain experienced a sharp surge in reported STI cases: gonorrhea increased by 49%, HIV by 45%, chlamydia by 39%, and syphilis by 32%. A similar pattern was observed in England, where health authorities recorded a pronounced and widespread increase in gonorrhea diagnoses, particularly among people aged 15–24.
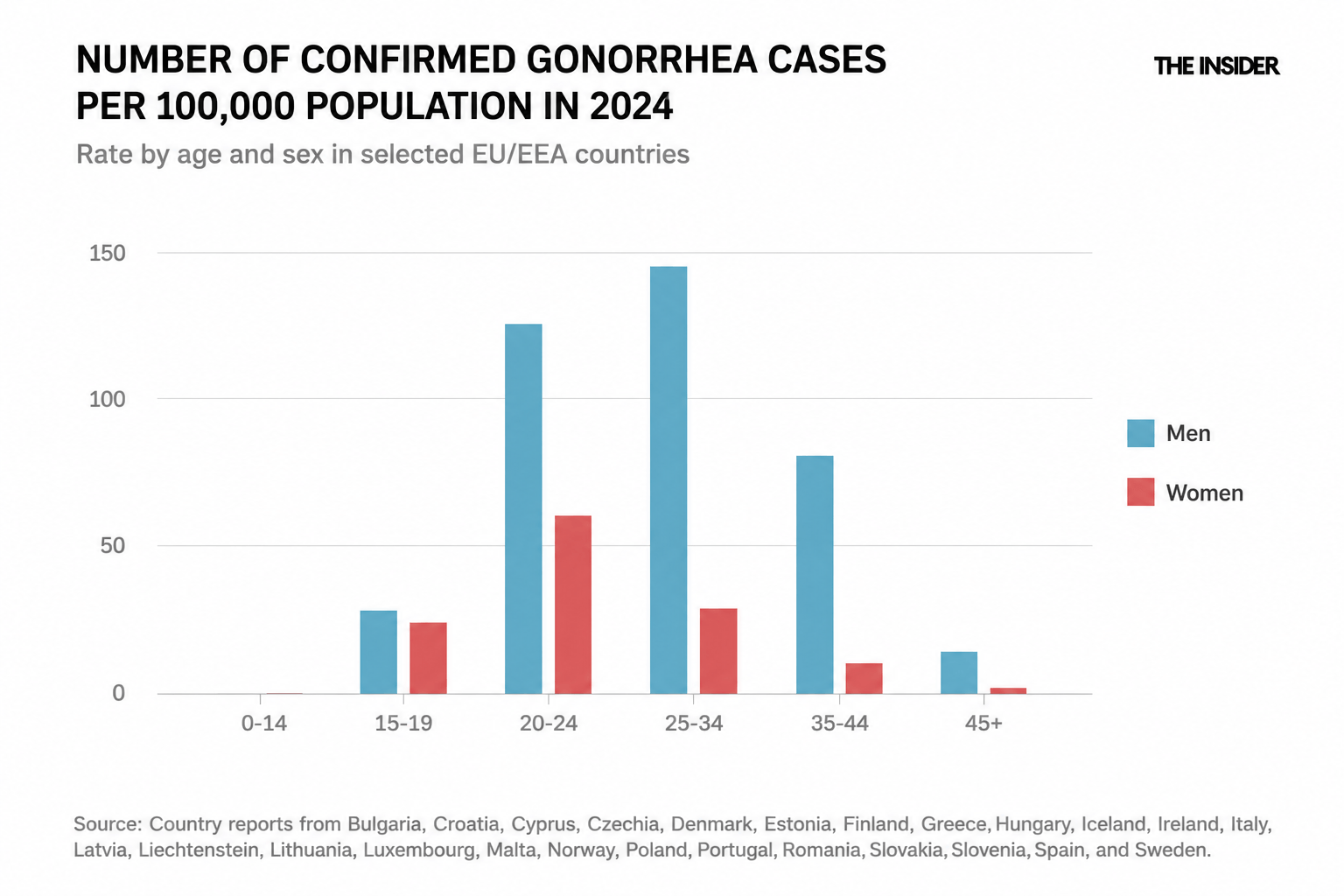
Importantly, the post-pandemic rise was not limited to traditionally high-risk groups. Among young people — especially women aged 20–24 — the reported rates of gonorrhea rose by nearly 200% between 2021 and 2023. The European Centre for Disease Prevention and Control attributes this trend to changes in sexual behavior during the post-pandemic period (even if the mechanisms behind this shift remain insufficiently understood).
Dating apps
The role of online dating platforms remains a frequently cited but difficult-to-verify factor. Such apps have dramatically lowered the barriers to finding sexual partners and may facilitate the formation of large sexual networks. However, it is statistically difficult to isolate their independent contribution to STI transmission dynamics.
App use correlates with a wide range of other behavioral variables, and as tempting as it may be to single out this factor, the ECDC does not do so.
Overexposed and invisible: A portrait of the epidemic across groups
The current STI wave has emerged at the intersection of behavioral changes facilitated by new biomedical tools, the structural weakening of prevention systems, and the post-pandemic disruption.
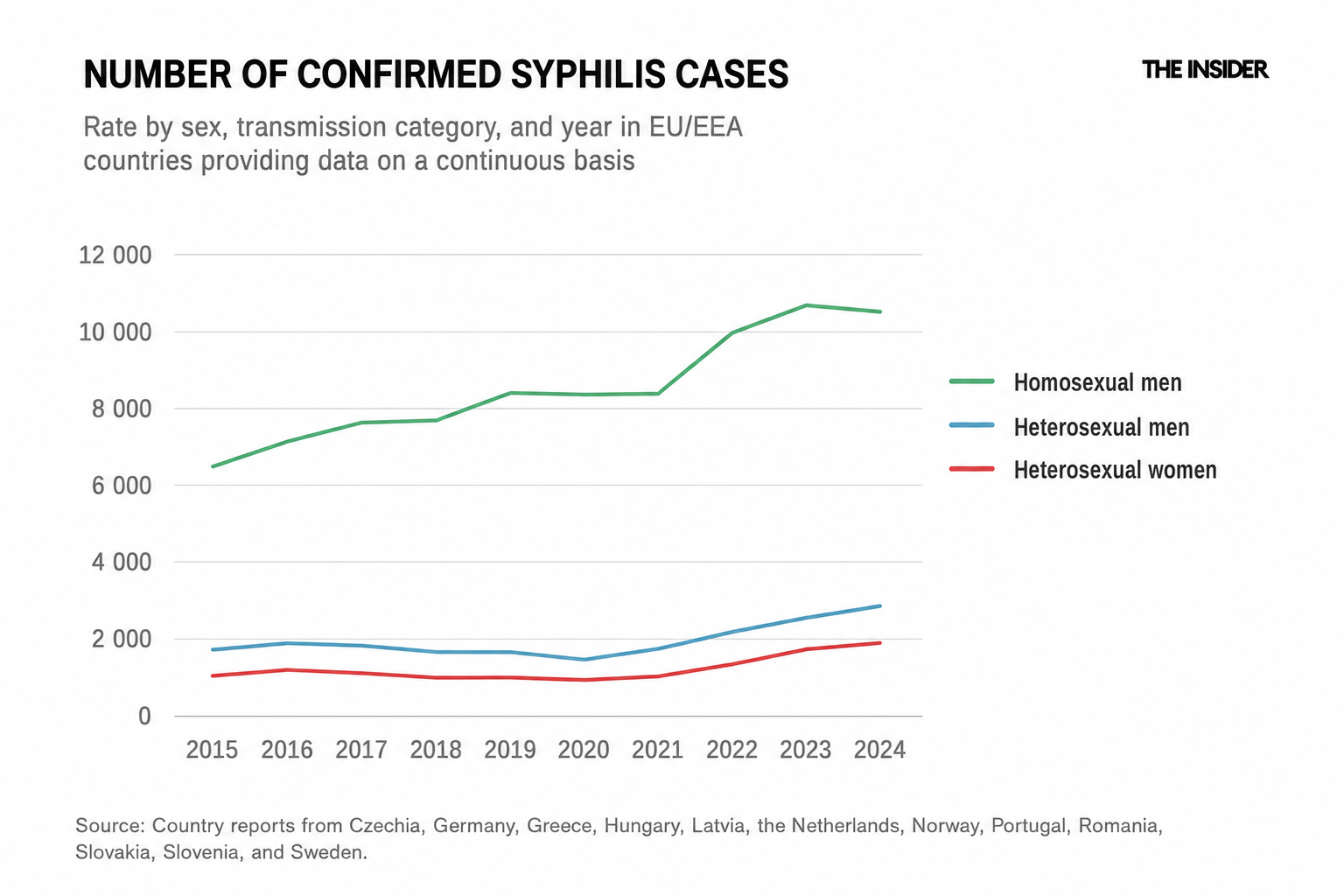
The first thing to note in the ECDC's reports is that MSM are disproportionately represented in European STI statistics. According to the ECDC, they account for 62% of gonorrhea cases and 69% of syphilis cases reported across the EU/EEA. Does this mean that MSM experience these infections seven times more often than the rest of the population? Not necessarily. More likely, they are tested at higher rates than members of other groups.
PrEP monitoring protocols require mandatory STI testing every three months, and in most European countries this schedule is embedded in national guidelines. Of the 29 EU/EEA countries that submitted data to the ECDC's 2024 monitoring program, 19 have policies mandating regular asymptomatic screening for all three major bacterial STIs among PrEP users. Because MSM are considered a higher-risk group, they receive greater medical attention. As a result, they are, in a sense, overrepresented in surveillance data.
The concentration of cases in certain countries supports this interpretation. Spain, the Netherlands, Germany, and France account for a disproportionately large share of Europe's gonorrhea and syphilis cases. These countries exhibit a specific combination of factors: well-developed PrEP infrastructures, high rates of chemsex among PrEP users, active LGBTQ+ tourism, and open sexual health systems with low barriers to care. The result is exceptionally high case detection. Spain, with 11,556 syphilis cases, and Germany, with 9,509 cases in 2024, lead the European statistics.
Against the backdrop of MSM data, the statistics for women appear much more reassuring: 69% of syphilis cases in the EU are reported among men and only 31% among women. This distribution is often interpreted as evidence that women are less affected by the disease.

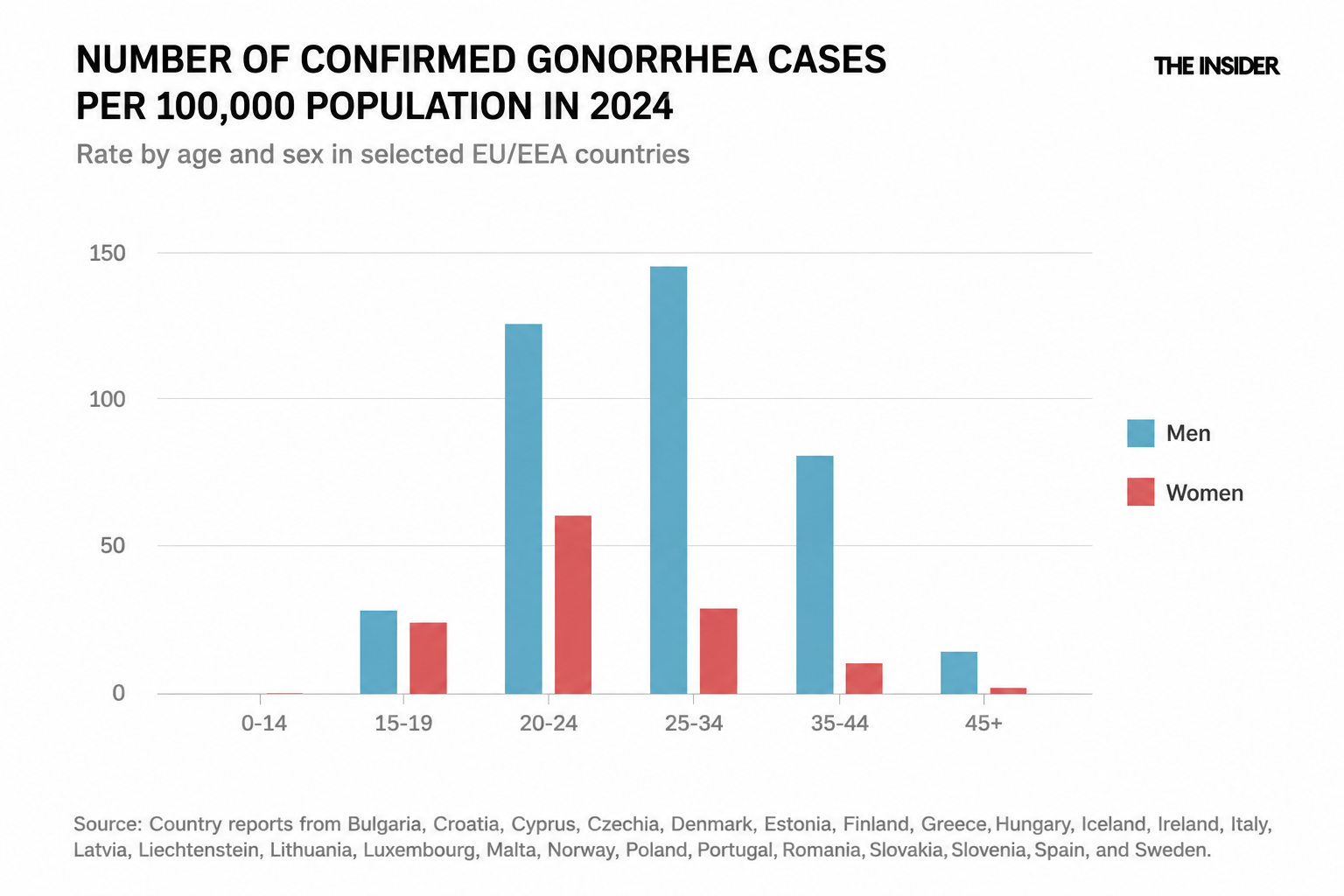
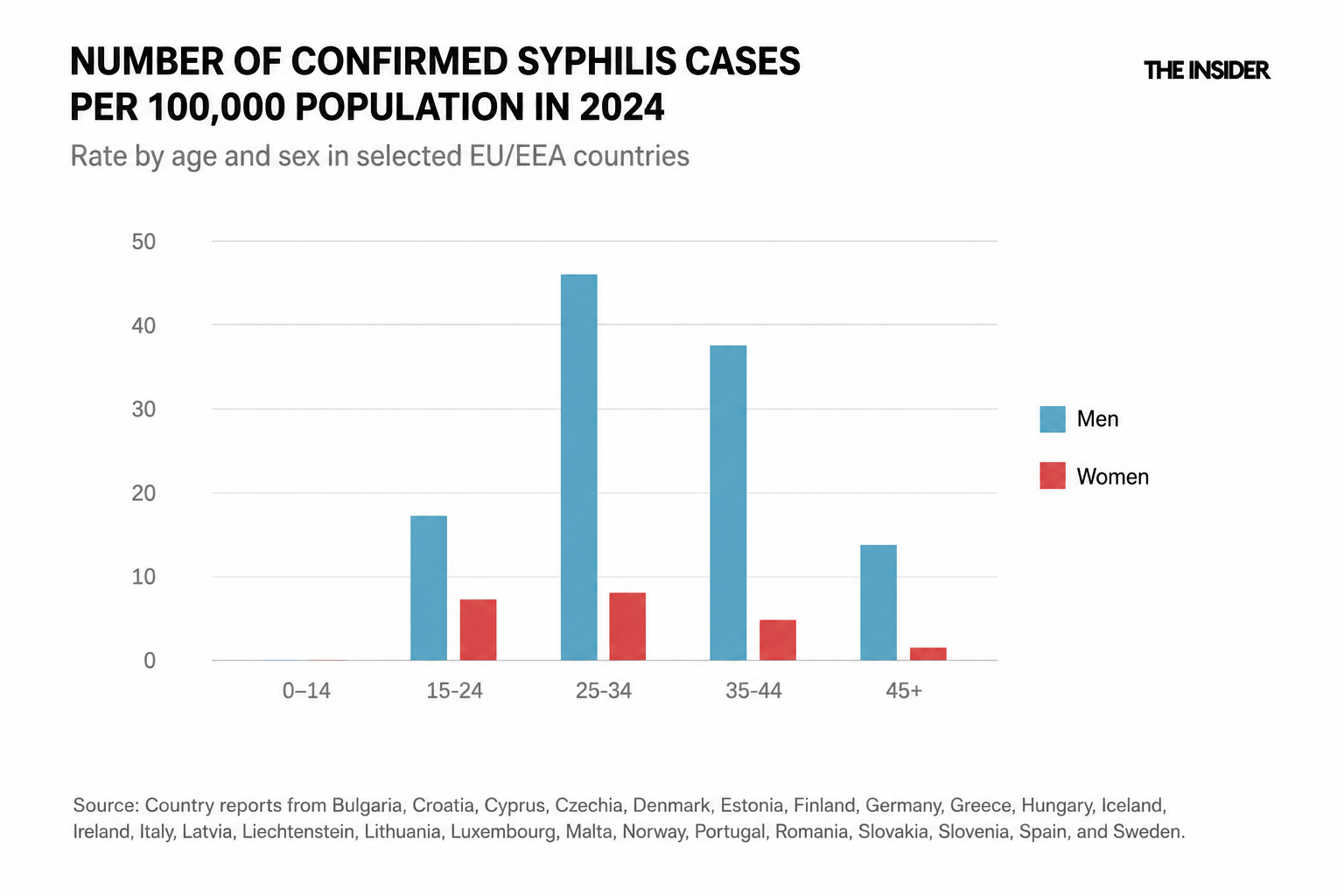
However, these statistics may be influenced by the fact that infections are detected less frequently in women, as well as by the way STIs manifest in female patients. Gonorrhea and syphilis in women are asymptomatic or present with only mild clinical symptoms in 50–80% of cases.
In most instances, a woman infected with gonorrhea will experience no symptoms that would prompt her to seek medical care. This means that symptom-driven testing — the primary route of case detection for most adults — works poorly for women. The only reliable way to determine the true burden of disease is to actively include women in screening programs, particularly during pregnancy.
Of the 29 EU/EEA countries that provided data to the ECDC, 27 have policies requiring syphilis screening during the first trimester of pregnancy — often, this is the only routine point of contact women have with STI testing systems. Outside pregnancy, routine STI screening for women does not exist in most European countries. Testing is typically ordered when symptoms appear or on an individual basis, but not systematically — unlike the situation for MSM.
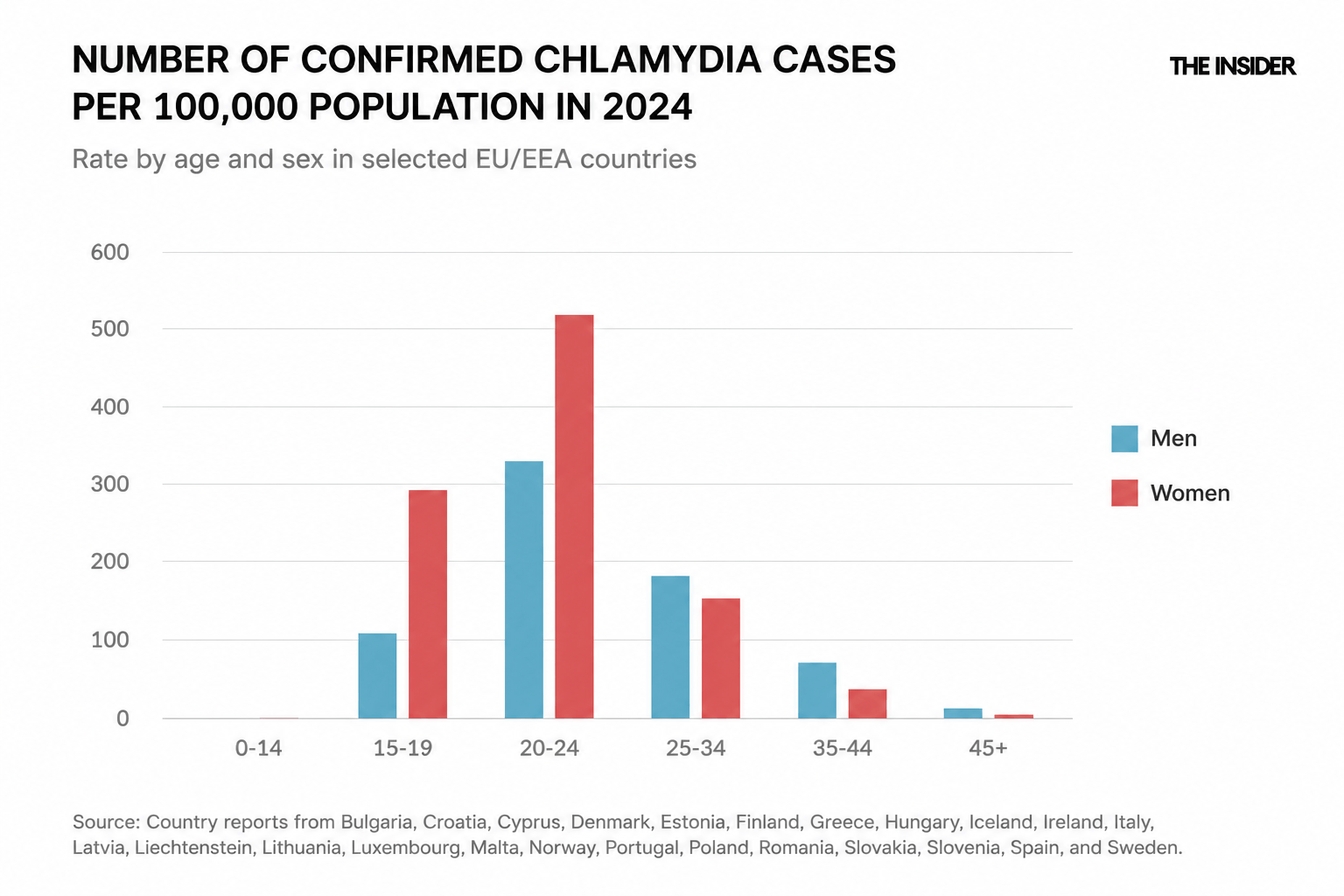
Chlamydia is an exception. According to the ECDC, chlamydia is detected far more frequently in women than either syphilis or gonorrhea, and women are nearly at parity with men in reported cases. This is largely because chlamydia has long been incorporated into gynecological screening programs in many countries.
Congenital syphilis statistics have also begun to rise, and their distribution across Europe is far from uniform. According to the ECDC, four countries — Hungary, Bulgaria, the Netherlands, and Portugal — account for a disproportionately large share of all reported cases in the EU/EEA.
Bulgaria has recorded the highest number of congenital syphilis cases. The infection is concentrated primarily within the Roma community. Although Roma account for only 4% of the population, they represented 35% of all syphilis cases identified in the study. More than half of those infected (55%) were women, and 14% of them were pregnant.
This is a population with limited access to healthcare, a high degree of social exclusion, and chronic distrust of state institutions. As a result, prenatal screening programs that could interrupt vertical transmission often fail to reach them.
A similar pattern can be observed in the Netherlands among migrant women working in the sex industry. Researchers at the Dutch Ministry of Health have documented substantially higher rates of syphilis in this group than among Dutch-born women. At the same time, they are far less likely to return for follow-up care. In other words, infections are detected but not systematically monitored, leaving treatment outcomes unknown.
The situation in Portugal is particularly troubling. The country has one of the highest national rates of congenital syphilis in Europe — 17.5 cases per 100,000 live births. This far exceeds the World Health Organization's elimination target, which requires a rate of no more than one case per 100,000 live births. To prevent mother-to-child transmission as effectively as possible, the WHO calls for syphilis testing coverage among pregnant women to exceed 95%. Portugal falls short of this target, with coverage gaps of around 50% among vulnerable population groups.
Women from marginalized communities, migrant women (the ECDC report notes that more than half of pregnant women diagnosed with syphilis in Portugal were born outside the country), and low-income women often do not receive prenatal care early in pregnancy and lack access to treatment.
Another almost entirely invisible group is victims of human trafficking. By definition, no comprehensive European data exist for this population: these are people who are being deliberately hidden from institutions, including healthcare systems. The limited studies available in the literature report STI rates among trafficking victims that are between 22 and 111 times higher than those observed in the general population. However, since this group falls outside registries and screening programs, its contribution to overall disease trends cannot be reliably estimated.
A detection crisis
From a medical standpoint, STIs have long ceased to be a particularly complex problem. The main treatment — benzathine penicillin — has been used for decades and remains the gold standard of therapy. STIs are relatively easy to diagnose, and in the case of syphilis, mother-to-child transmission can be prevented through timely testing and treatment during pregnancy. As a result, the current rise in STI rates is increasingly viewed not only as a medical issue but also as an organizational one.
Data from the ECDC show that STI prevention systems across Europe remain highly uneven. Of the 29 EU and European Economic Area countries that submitted data for the 2024 monitoring exercise, nearly half continue to charge at least part of the population a fee for STI testing.
Meanwhile, PrEP users typically undergo routine screening every three months as part of their medical follow-up, whereas for other groups access to testing depends on national healthcare systems and insurance coverage arrangements.
A similar situation exists when it comes to congenital syphilis prevention programs. Fifteen European countries do not have policies requiring repeat syphilis testing during the third trimester of pregnancy for women in high-risk groups. Only a handful of countries were able to provide complete data on screening uptake among pregnant women. And even fewer could supply accurate statistics on actual screening coverage. ECDC experts explicitly describe a critical reporting gap that makes it impossible to identify failures in the system in time to prevent transmission of the infection to newborns.
The problems extend beyond diagnostics. In recent years, eight European countries have reported shortages of benzathine penicillin, and shortages of this critically important medication are linked to vulnerabilities in global supply chains, particularly dependence on China.
At the same time, many national STI prevention strategies have been updated more slowly than recommended by international organizations. The WHO’s “Global Health Sector Strategies on HIV, Viral Hepatitis, and STIs” set an interim goal of updating and adapting national guidelines and programs in all participating countries by the middle of the decade. However, ECDC monitoring found that most countries still rely on outdated policy documents or address STIs only as a secondary component of broader HIV programs. This dilutes the focus on bacterial STIs and reduces funding dedicated to combating them.
Many of the measures that experts consider most effective do not require technological breakthroughs. These include expanding access to testing, introducing repeat screening for pregnant women in high-risk groups, integrating STI diagnostics into routine healthcare, and reaching populations that are less likely to engage with healthcare systems. According to experts, prevention and early detection are far less costly than treating the severe complications that can result from these infections.
Prevention and early detection of infection are far less costly than treating severe complications of disease
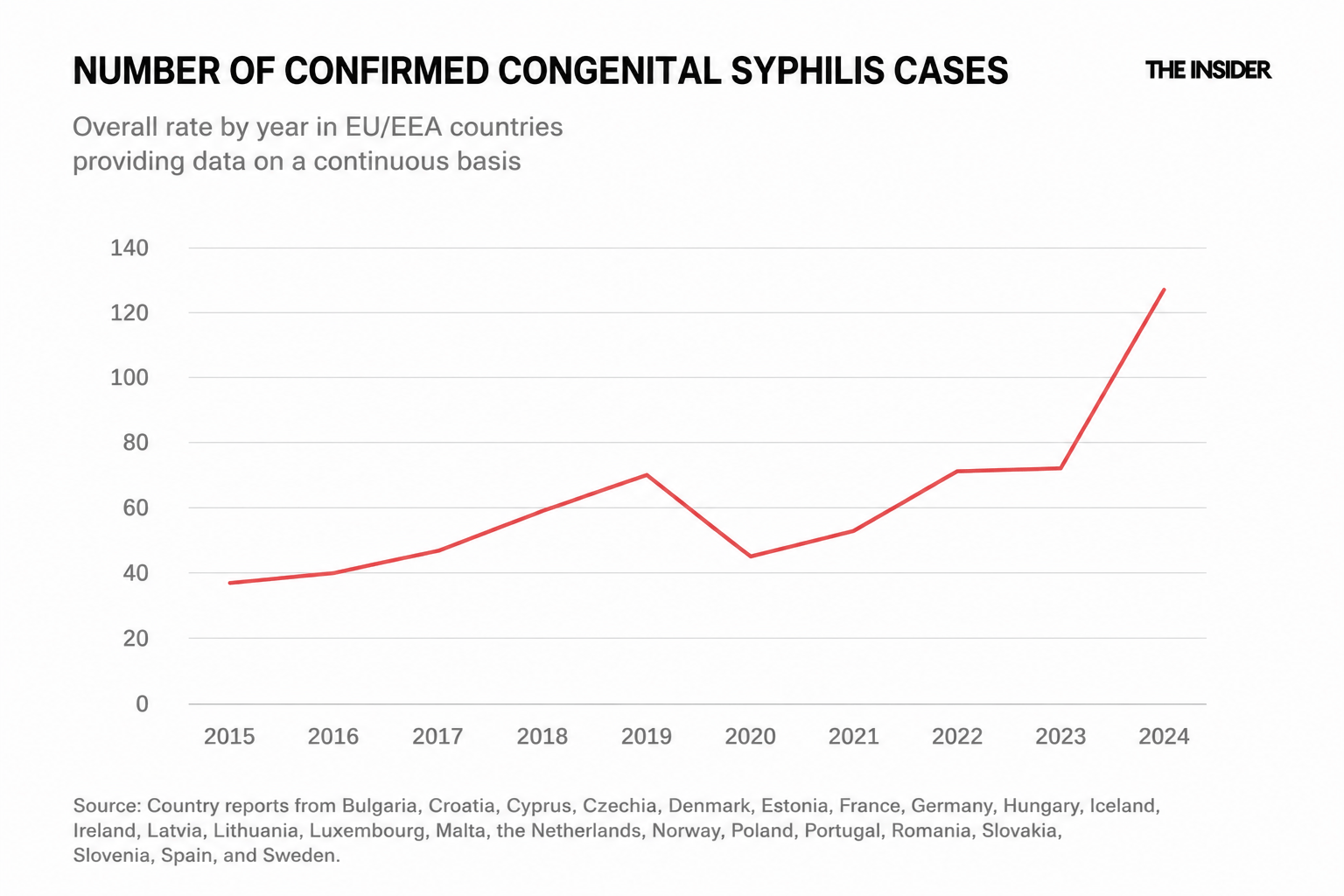
This is why, amid the broader rise in STI rates, the ECDC considers the increase in congenital syphilis cases to be the most alarming finding in the 2024 data. The number of reported cases in the EU/EEA rose from 78 in 2023 to 140 in 2024 — nearly doubling in a single year and reaching the highest level recorded since European surveillance began in the 1990s.
In modern medicine, such cases are often viewed not only as medical events but also as indicators of how well a healthcare system is functioning. Behind each diagnosis typically lies a chain of missed opportunities — delayed testing, late entry into prenatal care, or lack of access to healthcare services.
